The annual World Alzheimer’s Day has arrived. Every year on September 21, the world observes this day to raise awareness about Alzheimer’s disease (AD). Today, let’s take a closer look at the key features of Alzheimer’s, how to detect and diagnose it earlier, and how we can minimize the damage it causes. When we hear that an elderly person has “dementia,” in most cases it actually refers to AD, since Alzheimer’s disease is the leading form of dementia. Patients with AD exhibit large accumulations of amyloid-β (Aβ) plaques and neurofibrillary tangles (NFTs) in the brain, along with a series of pathological processes such as neuroinflammation, synaptic dysfunction, mitochondrial and bioenergetic disturbances, and vascular abnormalities. These ultimately contribute to neuronal death. Clinically, the main hallmark of Alzheimer’s is amnestic cognitive impairment. Early symptoms may include depression, anxiety, social withdrawal, and sleep disturbances. As the disease progresses, symptoms worsen, leading to severe memory loss, hallucinations, delusions, and other neuropsychiatric symptoms, which further exacerbate behavioral and emotional problems in the later stages. Some patients with non-amnestic forms of impairment may experience deficits in visuospatial skills, language, executive function, behavior, or motor skills. Unfortunately, there is still no cure for AD. Many patients are diagnosed at late, irreversible stages, with an average survival time of 4–8 years. Pathological changes in the brain actually begin decades before clinical symptoms appear. Typically, patients progress to mild cognitive impairment (MCI) within 6–10 years. About 15% of MCI patients convert to AD within 2 years, and roughly one-third progress within 5 years. This highlights the importance of focusing on the preclinical and MCI stages, where early intervention and management of modifiable risk factors may reduce the likelihood of developing AD or delay its progression. With advances in biomarkers and imaging technologies, researchers have developed sensitive tools for detecting AD pathology. Biomarkers such as Aβ, tau, neuroinflammatory proteins, and indicators of neuronal dysfunction in blood and cerebrospinal fluid, as well as the plasma Aβ42/Aβ40 ratio and phosphorylated tau (pTau), show promise for early diagnosis and prediction of cognitive decline. Imaging methods such as FDG-PET (for detecting metabolic activity) and MRI (for measuring brain atrophy) are also powerful techniques for diagnosing early AD. Overall, the causes of Alzheimer’s disease are complex and not yet fully understood. Beyond the critical roles of Aβ and tau proteins, a range of other factors may also drive AD pathology—forming the foundation for diagnostic and therapeutic strategies. Biomarkers can help identify patients early, monitor disease progression, and evaluate treatment efficacy. Hypotheses centered on these pathogenic mechanisms provide potential drug targets. However, developing effective Alzheimer’s therapeutics remains a great challenge. It is our hope that scientists and physicians worldwide will continue working together to gain deeper insight into the mechanisms of AD, discover more precise diagnostic markers, and develop truly effective treatments. Research on AD relies heavily on the development of animal models. Brain Case Biotech can assist you in constructing tau overexpression AAV vectors and also provide experimental services for generating AD mouse models. If you are interested, please feel free to contact us at bd@ebraincase.com.
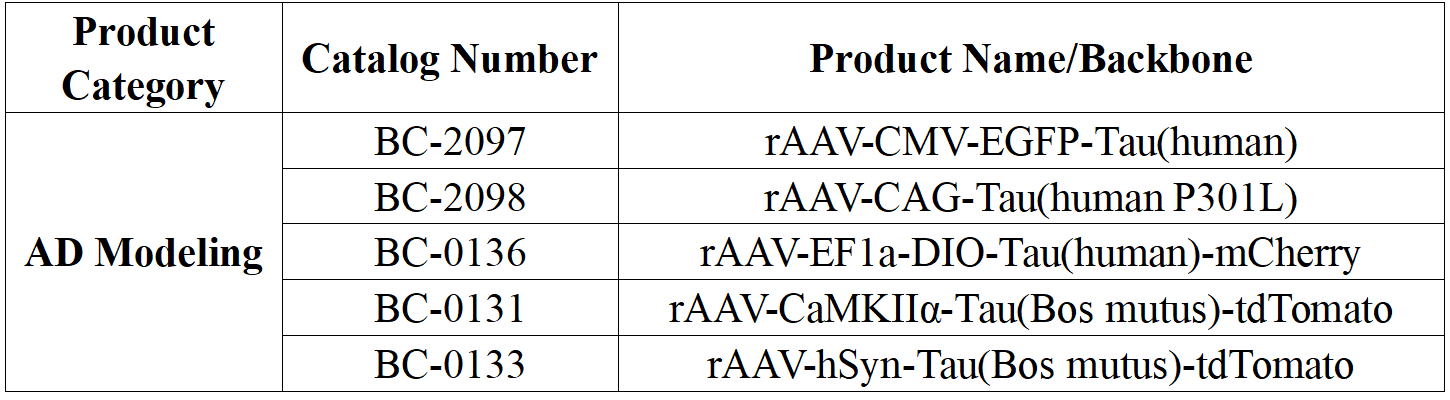
In AD research, adeno-associated virus (AAV) is commonly used as a vector to deliver AD-related pathological genes, such as APP mutant genes and Tau mutant genes, into the brains of experimental animals (e.g., hippocampus, cortex). This induces β-amyloid deposition, Tau aggregation, and cognitive impairments, creating animal models that closely mimic AD pathology and phenotypes for mechanistic studies and drug screening.
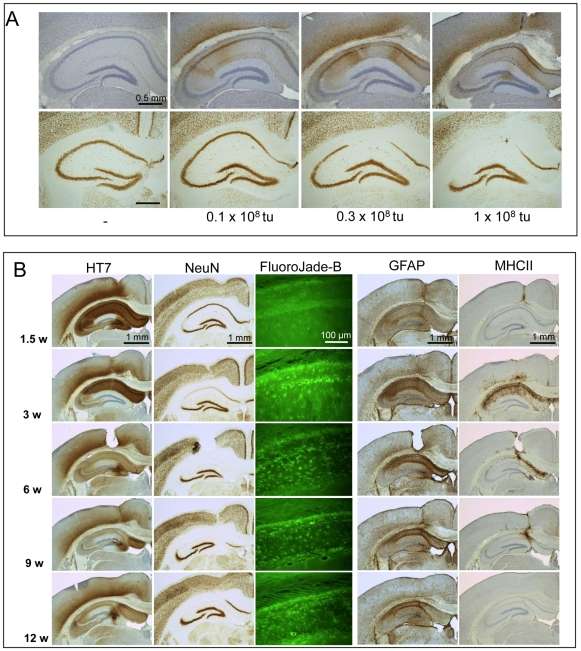
1. AAV-mediated Tau protein expression induces degeneration of pyramidal neurons in wild-type mice via cell cycle re-entry without forming neurofibrillary tangles •Experimental animals: Wild-type FVB/N mice •Virus name: rAAV1/2-hSyn-hTau (P301L) •Injection scheme: Stereotaxic injection into hippocampus, 1.0 × 10⁸ vg, expression for 12 weeks •Experimental results: Injection of AAV-Tau (P301L) into the mouse brain at low doses caused mild neurodegeneration, with thinning of the hippocampal CA1/2 region. As neuronal loss increased, hTau expression decreased due to reduced protein synthesis in degenerating neurons. Lesions appeared first in the CA2 region at 1.5 weeks post-injection, progressed to CA1 by 3 weeks, and by 6–12 weeks, most pyramidal cells in the CA regions were lost and degeneration extended to the cortex. Fluoro-Jade B (FJB) staining indicated degenerating neurons. Microglial activation was transient at later stages, disappearing by 12 weeks, while astrocytes remained activated, indicating inflammation. Control mice injected with AAV-EGFP showed no neuronal loss or microglial activation. AAV-Tau-P301L induced degeneration of pyramidal neurons in the hippocampal CA regions and cortex, and microglial activation was specifically associated with Tau-mediated neurodegeneration, not with amyloid, viral particles, or viral protein responses.
Figure 1. Dose-dependence and timeline of AAV-Tau P301L–mediated neuronal degeneration
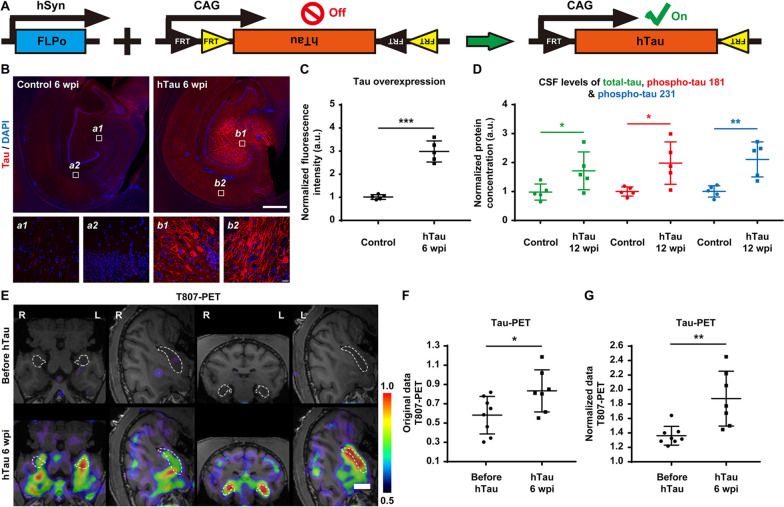
2. Construction of a non-human primate (NHP) model with Alzheimer’s disease-like pathology via hippocampal overexpression of human tau protein
• Animal model: Adult rhesus monkeys (7–15 years old)
• Virus name: rAAV9-hTau (WT)
• Injection scheme: Bilateral stereotaxic hippocampal injection, 10¹⁰–10¹¹ GC, expression 6–12 weeks / 50 weeks
• Experimental results: To generate a non-human primate model with Tau protein–induced AD-like pathology, adult rhesus monkeys (7–15 years old) were stereotaxically injected with AAV vectors overexpressing hTau. Multiple detection methods including immunostaining and PET/MRI imaging were used. Results showed an AAV-mediated gene transduction efficiency of approximately 75%, with stable expression maintained from 6 to 50 weeks, indicating that AAV effectively induces widespread and persistent Tau protein expression.
Figure 2. Stereotaxic bilateral hippocampal injection of AAV achieves sustained Tau overexpression in NHP model
Reference Zhang J, Zhang Y, Wang J, Xia Y, Zhang J, Chen L. Recent advances in Alzheimer’s disease: Mechanisms, clinical trials and new drug development strategies. Signal Transduct Target Ther. 2024 Aug 23;9(1):211. doi:10.1038/s41392-024-01911-3. PMID:39174535; PMCID:PMC11344989. Self WK, Holtzman DM. Emerging diagnostics and therapeutics for Alzheimer disease. Nature Medicine. 2023 Sep;29(9):2187-2199. doi:10.1038/s41591-023-02505-2. PMID:37667136. Jaworski T, Dewachter I, Lechat B, et al. AAV-tau mediates pyramidal neurodegeneration by cell-cycle re-entry without neurofibrillary tangle formation in wild-type mice. PLoS One. 2009;4(10):e7280. Jiang Z, Wang J, Qin Y, et al. A nonhuman primate model with Alzheimer's disease-like pathology induced by hippocampal overexpression of human tau. Alzheimers Res Ther. 2024;16(1):22.
Service Type :
Select the service you'd like to purchase.
Order Information(Premade-AAVs)
Please provide us some information about the service you'd like to order.
Order Information(Custom AAV/Lentivirus)
Please provide us some information about the service you'd like to order.
Order Information(Others)
Please provide us some information about the service you'd like to order.